
The long-standing chasm between federal and state marijuana policy recently widened when U.S. Attorney General Jeff Sessions rescinded Obama-era guidance indicating that the Justice Department would not make it a priority to prosecute federal marijuana crimes in states where the activities are legal. At present, a budgetary amendment is the only legal barrier to Justice Department enforcement of the Controlled Substances Act (CSA) against users and sellers of medical marijuana in the 30 states that have legalized it. Nothing prevents federal prosecution of recreational marijuana activities in jurisdictions where they are legal. However, spurred by Sessions’s policy, Senator Elizabeth Warren (D-MA) introduced a bipartisan bill in June 2018 (S.3032) that would exempt most marijuana-related activities from CSA application when they’re allowed under state or tribal law — legislation that President Donald Trump says he will support. As the marijuana-policy terrain shifts, it’s important to consider the potential public health benefits of closing the federal–state divide.
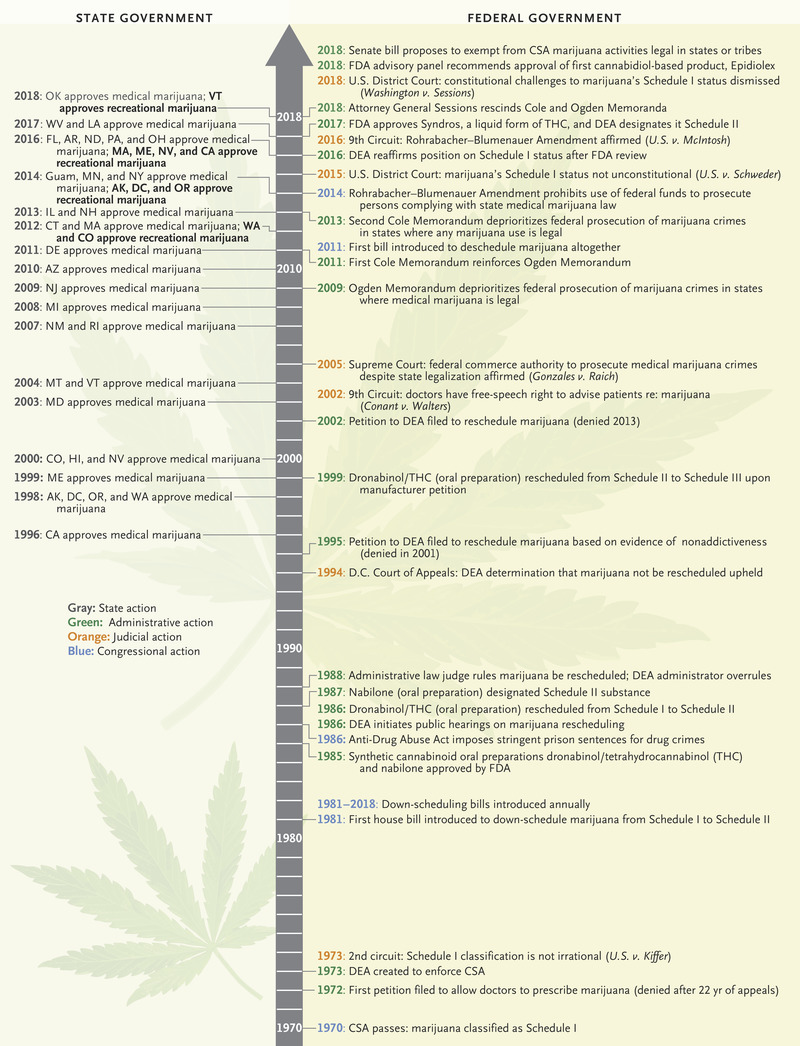
U.S. Marijuana Policy Milestones, 1970–2018.
Controversy over marijuana policy originates from the 1970 federal decision to classify marijuana as a Schedule I substance under the CSA. Schedule I drugs are deemed to have high potential for abuse and no accepted medical use. Crimes involving such drugs can result in penalties of thousands to millions of dollars and substantial prison time. Marijuana’s Schedule I classification has been repeatedly challenged in all branches of the federal government (see timeline), but although synthesized versions of some marijuana components, including the psychoactive compound tetrahydrocannabinol (THC), have been rescheduled and approved by the Food and Drug Administration (FDA), the plant as a whole has not. The FDA did recently approve a plant-based product, cannabidiol (CBD; Epidiolex), for the treatment of certain seizures in children.1 The Drug Enforcement Administration is expected to reschedule CBD so that Epidiolex can be sold legally.
Although the Obama administration did not support rescheduling of marijuana, it signaled in a series of Justice Department memos that it would ease federal marijuana-crime enforcement in some circumstances. This guidance culminated in the 2013 Cole Memorandum, which deprioritized marijuana prosecutions in states where use was legal, indicating that states could proceed with carefully regulating and taxing marijuana. The Rohrabacher–Blumenauer Amendment (previously the Rohrabacher–Farr Amendment), adopted by Congress the following year and currently renewed through September 2018, went further, prohibiting the use of federal funds to prosecute medical marijuana activities.
Encouraged by these developments, states have moved toward marijuana legalization, which more than 6 in 10 Americans now favor, according to a survey by the Pew Research Center. Starting with California in 1996, more than half the states have legalized medical marijuana, and at least three are currently considering doing so. This year, at least six more states are poised to follow the nine states and District of Columbia that have legalized recreational marijuana.
As state legal restrictions have eased and evidence concerning marijuana’s medical benefits has accumulated, marijuana use has increased: about 9% of Americans 12 years of age or older used marijuana in 2016, according to the National Survey on Drug Use and Health. Marijuana sales in states where they are legal topped $8 billion in 2017 and are projected to grow to $24 billion by 2025.2 State revenues from taxes and permits — totaling $745 million in 2017 and used for budget shortfalls, schools, public heath, and law-enforcement programs — are expected to reach $4.3 billion in 2020.2 In short, state marijuana legalization and industry growth show no signs of slowing.
Sessions’s about-face in January introduced new uncertainty. Although marijuana taxes typically account for at most 1% of state general-fund revenues, states’ reliance on this money may increase as sales grow. Marijuana businesses face difficulty obtaining federally regulated credit and other banking services because of their precarious legal status.3
Such effects could jeopardize the continuity of the medical marijuana supply. In some states, dispensaries are licensed to supply to both recreational and medical users, so action against them or their suppliers shrinks access for all. For patients using marijuana in lieu of potentially riskier alternatives such as opioids, supply reductions could worsen health outcomes. Furthermore, marijuana’s Schedule I status is a known hindrance to conducting the research required to secure FDA approval of medical marijuana products; federal funding for such research has been meager, and the federal government has a monopoly on supplying marijuana for clinical trials.
 Another threat to medical users is the possibility that Congress will not renew the Rohrabacher–Blumenauer Amendment, leaving prescribers, dispensers, and patients vulnerable to federal criminal enforcement. Ultimately, individual U.S. attorneys’ offices will have to decide how to prioritize prosecution of federal marijuana offenses in light of competing demands on their resources — which will exacerbate the unpredictability of marijuana markets. U.S. attorneys have considerable discretion, and though the social climate for prosecuting medical users in particular is not favorable, there are no longer any guarantees.
Another threat to medical users is the possibility that Congress will not renew the Rohrabacher–Blumenauer Amendment, leaving prescribers, dispensers, and patients vulnerable to federal criminal enforcement. Ultimately, individual U.S. attorneys’ offices will have to decide how to prioritize prosecution of federal marijuana offenses in light of competing demands on their resources — which will exacerbate the unpredictability of marijuana markets. U.S. attorneys have considerable discretion, and though the social climate for prosecuting medical users in particular is not favorable, there are no longer any guarantees.
In addition, the absence of a sensible, stable federal marijuana policy affects the safety of marijuana products and physicians’ comfort in recommending or prescribing them. Although the FDA has an approval track for botanicals, only one purified plant-based marijuana product is currently regulated by the FDA.1 Inconsistency in marijuana regulation from state to state can allow inappropriate marketing, formulation, and packaging practices to persist — making THC content across samples unpredictable, for instance, or permitting marketing of edibles that appeal to children.4 Without FDA approval, a lack of information about efficacy, dosing, adverse effects, and availability of marijuana products deters providers from recommending them.
The present state of conflicting laws seems unstable and suboptimal for rational drug control. Federal regulation that accommodates and reinforces state medical marijuana regulatory regimes would result in a safer, more reliable, more accessible supply of marijuana products. Congress, because it answers to the people and represents the states, appears the most likely branch to move on marijuana policy; it could even be encouraged to act by Canada’s recent legalization of recreational marijuana. Federal courts are increasingly hearing challenges to marijuana’s Schedule I status but have so far been unwilling to deem Congress’s scheduling determination irrational and therefore unconstitutional.
In Congress, rescheduling marijuana by amending the CSA is one attractive option. The executive branch, too, can reschedule CSA substances,3 but the mechanisms are time consuming and unlikely to attract interest within the current administration. Because considerable evidence now supports marijuana’s therapeutic benefits in reducing chronic pain, nausea, and vomiting in patients with cancer, as well as multiple sclerosis–related muscle spasms,5 there is a compelling argument that marijuana is more appropriately designated as a Schedule II or Schedule III drug. Rescheduling would facilitate further study of products for FDA approval, but would not automatically change the severity of penalties for marijuana crimes or alter international treaty obligations, enshrined in the CSA, to ensure that all psychoactive substances are used only for legitimate medical and scientific purposes.3
Congress could also remove marijuana from the CSA schedules altogether. This dramatic action could be coupled with legislation authorizing FDA oversight of marijuana products. Whether marijuana’s psychoactive effects preclude this move away from regulation as a controlled substance would provoke considerable debate. Subjecting marijuana products to FDA approval would hinder access initially but ultimately foster a robust system for regulation and research. FDA oversight of marketing would also improve product safety and consistent promotion across states.3
The Warren legislation represents a third option designed to respect states’ rights — codifying the approach articulated in the Cole Memorandum by amending the CSA to exempt marijuana activities that are lawful in the jurisdiction where they occur. This solution would be more permanent than attorney-general guidance or agreements between states and the attorney general regarding enforcement, which shift with the political winds, and would therefore promote stability for medical users and suppliers. But it would not facilitate research into marijuana harms and benefits, bring products within the FDA’s purview to ensure safety and efficacy, alleviate interstate health risks, or address potential conflicts with international treaty obligations.
We think this third option, which addresses some pressing conflict-of-law concerns such as unpredictable criminal enforcement, is preferable to the current blurred vision of the future of marijuana policy. Ultimately, a more comprehensive federal regime that perhaps resembles Canada’s recent legalization of recreational marijuana could affirmatively promote health and safety through research and regulation.
